the posterior wrist tendons are separated into 6 compartments.
- compartment 1: abductor pollicus longus (apl) and extensor pollicis brevis (epb).
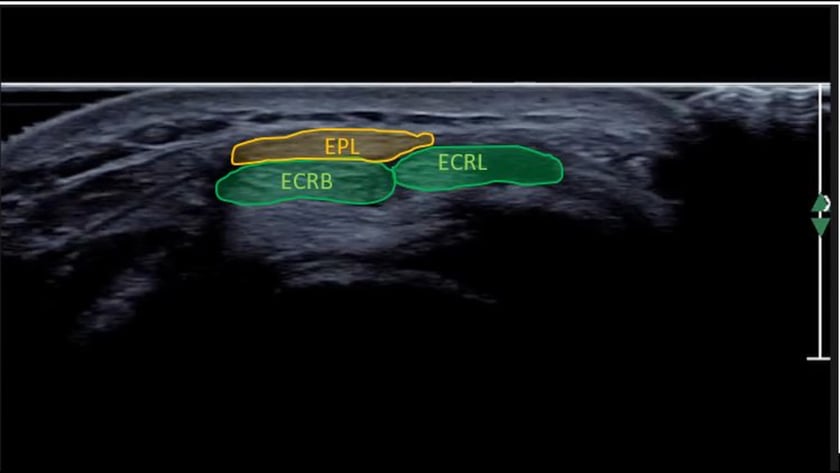
- compartment 2: extensor carpi radialis longus &extensor carpi radialis brevis.
- compartment 3: extensor pollicis longis.
- compartment 4: extensor digitorum
- compartment 5: extensor digiti minimi.
- compartment 6: extensor carpi ulnaris.
other posterior wrist structures to assess.
- wrist joints (particularly the dorsal recess)
- scapho-lunate ligament.
- proximal intersection (compartment 1 over compartment 2)
- distal intersection (compartment 3 over compartment 2)

to assess the tendons:
- scan each tendon in transverse from the musculo-tendonous junction to the mid hand.
- rotate into longitudinal and mobilise each tendon to ensure it is intact and glides freely.
tip: rest the patient's wrist over a rolled towel gentle flexed to create tension on the tendons.
normal appearances:
- the tendons should be echogenic and fibrillar.
- no fluid should be visible in the tendon sheaths.
- become familiar with the retinaculae overlying the tendons.
tip: the retinaculum overlying the extensor digitorum and extensor carpi ulnaris are thicker than the remaining retinaculae.
most common findings:
- fluid in tendon sheaths
- joint effusions (simple or complex)
- synovial thickening (tendon sheath or joint)
- increased vascularity.


- begin your scan at the wrist crease.
- initially, survey each tendon in transverse from the musculo-tendinous junction to the distal insertion.
- then assess in longitudinal also.
- the tendon sheaths approximately extend for a couple of cm either side of the wrist crease.
- if necessary, you can compare with the contralateral side.
posterior wrist

abductor pollicis longus(apl) and extensor pollicis brevis (epb)the posterior wrist is conveniently divided into 6 compartments:
- extensor carpi radialis (ecr) longus and brevis
- extensor pollicis longus (epl)
- extensor digitorum (ed)
- extensor digiti minimi (edm)
- extensor carpi ulnaris (ecu)
these are all tethered by the extensor retinaculum which overlies ,and in some areas reflects around, the tendons.
begin by scanning over the lateral wrist crease at the anatomical “snuff-box”. you should see the apl & epb in compartment 1. to check, both tendons should be able to be followed up the thumb. if they go to the carpus you have slipped medially onto compartment 2. work your way sequentially across the wrist assessing each tendon individually.
de quervain’s tenosynovitis
for pathology example images, click here to goto the wrist pathology page.
- inflammation of the abductor pollicis longus and extensor pollicis brevis tendons.
- overuse injury.
- patients present with focal, point tenderness laterally over the radial styloid.
proximal intersection syndrome
for pathology example images, click here to goto the wrist pathology page.
extensor pollicis brevis crossing over extensor carpi radialis longus & brevis.
distal intersection syndrome
for pathology example images, click here to goto the wrist pathology page.
ext pollicis longus crossing over extensor carpi radialis longus & brevis.
scapho-lunate ligament
for pathology example images, click here to goto the wrist pathology page.
the wrist is essentially divided into 3 joint planes:
1. and 2. the radiocarpal and midcarpal joints allow wrist flexion, extension and lateral deviation.
3. the distal radio-ulnar joint allows the forearm and hand to rotate. (pronation / supination).
these joints are supported by a series of extrinsic and intrinsic ligaments. the scapholunate ligament is the most important dorsal intrinsic stabiliser.
- injury occurs with a hyperextension of the wrist. similar mechanism to a scaphoid fracture but results in a ligament tear instead.
- if only a partial tear it is usually stable.
- if complete, it results in scapho-lunate instability. the scaphoid will rotate abnormally during wrist movement, which if left untreated can lead to significant chronic wrist degeneration.
note:
visualising the scl does not exclude carpal instability. (ref: ajr article )
anterior wrist

click image to enlarge
for pathology example images, click here to goto the wrist pathology page.carpal tunnel syndrome
this is the most common peripheral nerve entrapment. it occurs when the median nerve is compressed by the overlying flexor retinaculum.
important:
- ultrasound cannot exclude carpal tunnel syndrome. the accepted standard for diagnosis is a nerve conduction study.
- our role is to identify possible causes for the patient’s symptoms.
look for:
- tendon abnormalities
- ganglia
- fluid
- accessory muscles
- any asymmetry with the contra lateral side.
there have been several proposed methods of quatitative assessment for carpal tunnel. in our experience, these have not been reliable. they include:
- nerve cross sectional area of >10square mm proximal to the retinaculum.
- nerve flattening ratio of 3:1 (yesildag et al – clinical radiology).
guyons canal syndrome
for pathology example images, click here to goto the wrist pathology page.
canal bordered by the pisiform & hamate and roofed by a reflection of the flexor retinaculum. the ulna nerve and artery pass through and may become entrapped or injured. repetitive injury such as cycling or using heel of hand as hammer.
on ultrasound: as with carpal tunnel look for ganglia, accessory muscles and asymmetry with the contra lateral side
triangular fibrocartilage complex (tfcc)
for pathology example images, click here to goto the wrist pathology page.
- a section of cartilage and ligaments at the distal ulna.
- provides a continuous gliding surface along the forearm-carpal joint.
affected by:
- natural degeneration with age.
or injuries:
- foosh
- forced rotation (stuck drill)
- racquet sports
- direct blow to medial wrist