background
endometriosis is a common chronic gynaecological condition affecting approximately 1 in 10 female-born people. it manifests in three ways;
- superficial (peritoneal) endometriosis
- ovarian endometriosis (endometriomas)
- deep endometriosis (de)
superficial endometriosis will not be routinely detected via ultrasound but the presence of “soft markers” can indicate its existence.
de occurs when deposits of endometriosis penetrate >5mm below the surface of the peritoneum and is the most severe form of the disease.
indications
known or suspected endometriosis
chronic pelvic pain
dysmenorrhoea
dyschezia
dyspareunia
subfertility/ infertility
normal ultrasound anatomy
- uterus and ovaries (as for a routine pelvic ultrasound)
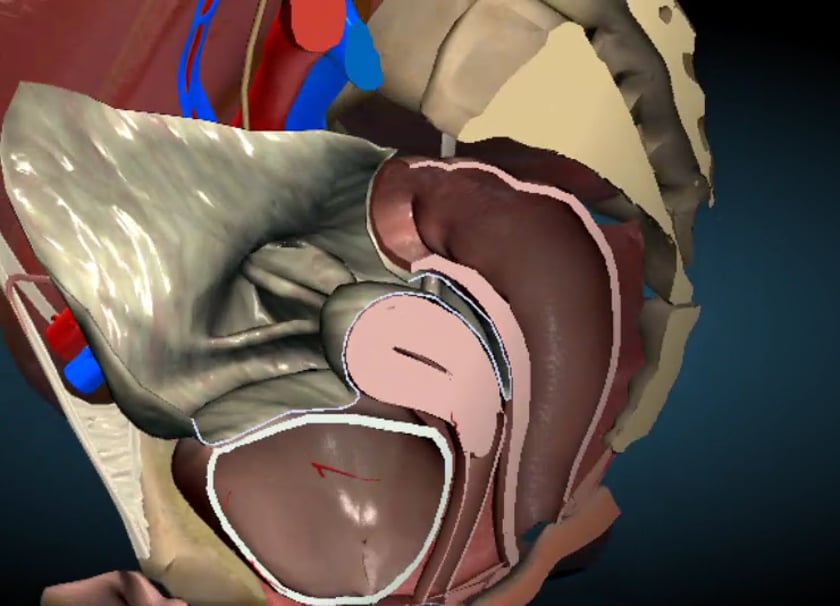
- anterior compartment
bladder
appears uniformly thin-walled
vesicouterine space
the potential space located between the anterior uterus and the posterior urinary bladder. in real-time these two structures should be seen to move apart with the sliding sign
ureters
hypoechoic tubular structures which are seen to vermiculate (i.e. contract to move urine from the kidneys to the bladder) in real-time 2
rectosigmoid colon
-the colon walls appear sonographically as an alternating hyper/hypoechoic layered structure 1
-the colon walls appear sonographically as an alternating hyper/hypoechoic layered structure 1
pouch of douglas (pod_
the use of the sliding sign 1 should reveal the pod to be open.
a small-to-moderate amount of free fluid in the pod is normal.
uterosacral ligaments
the normal uterosacral ligaments are seen as a very thin hyperechoic line or may not be seen at all. the midline joining point of the left and right uterosacral ligaments is the torus uterinus 2,3
posterior vaginal wall / posterior vaginal fornix
it is a thin, hypoechoic line directly posterior to the face of the transducer
rectovaginal septum
it is a thin, hyperechoic line between the hypoechoic posterior vaginal wall and the rectum 1,4
sonographic technique
pelvic ultrasound of endometriosis is an extension of a traditional transvaginal pelvic ultrasound. transabdominal imaging of little use in the assessment of deep endometriosis. the highest possible frequency transducer should be used. if required, a moderate amount of ultrasound gel (approx. 20 ml) can be instilled into the vagina or placed within the probe cover to use as a stand-off for assess the superficial structures of the posterior compartment but is not essential.
bowel preparation can be used to help visualise the bowel but is not essential.
the scan should be performed in four steps as proposed by the idea consensus statement 1:
- assessment of the uterus and ovaries
- assessment for ‘soft markers’ (ovarian mobility and site-specific tenderness)
- assessment of the sliding sign
- assessment of the anterior and posterior compartments
uterus and ovaries
this is done as per a traditional pelvic ultrasound. specific attention should be paid to the presence of adenomyosis or ovarian endometrioma. an anteverted/ retroflexed uterus has a strong association with adhesions in the posterior compartment 1.
assessment for ‘soft markers’ (ovarian mobility and site specific tenderness)
by applying gentle pressure with the transducer and the sonographers freehand on the abdomen, the ovaries can be seen to move in real-time. if mobility is reduced or not present, this can suggest adhesions.
the sonographer should take note of any sites which are tender when gentle pressure is applied.
assessment of the sliding sign
the sliding sign is assessed by using pressure with the transvaginal probe and the sonographers free hand to palpate the uterus over the abdomen to see the uterus/ cervix move away for the bowel.
the sliding sign is considered negative if the structures do not move freely and indicated that the pouch od douglas is obliterated.
assessment of the anterior and posterior compartments
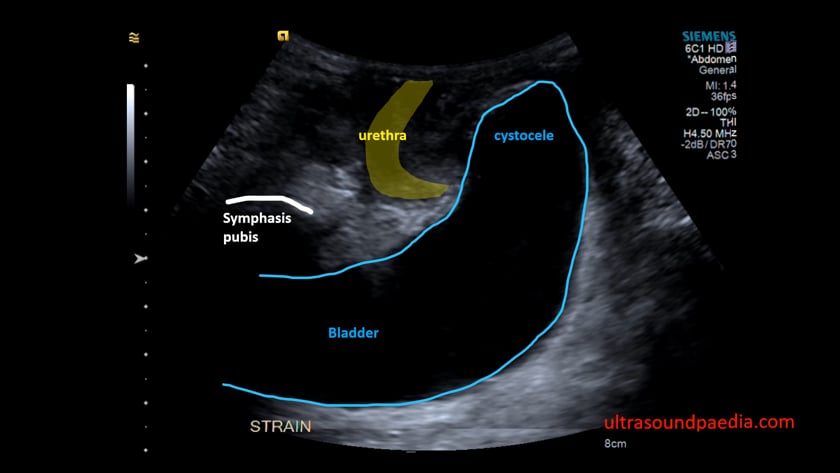
bladder
the bladder walls are difficult to assess without urine in the bladder
a full bladder, however, will hinder the view of other structures transvaginally 4 with the transducer in the anterior fornix, the probe is moved side to side, and cranial-caudal to assess the walls for nodularity.
if needed, the bladder can be assessed fully distended with a transabdominal scan.
vesicouterine space
with the transducer in the anterior fornix and the sonographers free hand placed over the suprapubic region, the posterior bladder should slide freely over the anterior uterine wall with pressure from both the transducer and the hand. 1
ureters
with the transducer in the anterior fornix, move laterally to visualise the vesicoureteric junction (vuj) at the bladder base and rotate slightly until the distal ureter can be seen running parallel to the bladder. the ureter can then be followed high into the pelvis.
in real-time, the ureters should be seen to vermiculate. 2
rectosigmoid colon
with the transducer at the opening of the vagina, trace the lower rectum until the transducer is in the posterior vaginal fornix; continue to follow the longitudinal plane of the rectosigmoid colon until it can no longer be visualised (usually past the level of the uterine fundus and left ovary); repeat in the transverse plane.
due to the normal twisting of the bowel, constant fanning and rotating of the transducer is essential to keep the bowel walls in view. 4
the view of the bowel may be hindered by the presence of mass lesions such as endometriomas or fibroids.
pouch of douglas (pod)
assess using the sliding sign – the posterior uterus and the anterior rectum should move apart freely with transducer pressure. 1
also, assess the pod for the presence of any nodules
uterosacral ligaments
with the transducer in the posterior fornix, move the transducer laterally and rotate slightly (30-45 degrees); the uterosacral ligaments will be seen in long axis as a thin white line immediately deep to the vaginal wall. 3,4
if the white line does not appear crisp (but heterogeneous in nature), the transducer is too lateral and imaging the parametrium. 3
in the transverse plane, within the transducer in the anterior vaginal fornix, the uterosacral ligaments can be seen immediately lateral to the cervix as the level of the internal os as they travel inferomedial to join at the torus uterinus.
when endometriosis is present, the uterosacral ligaments may appear thicker due to a thickening of the surrounding fat; a hypoechoic nodule may be present. 4
posterior vaginal wall / posterior vaginal fornix
the walls of the lower vagina are best assessed with the rectovaginal septum .
rectovaginal septum
endometriosis of the rectovaginal septum is rare, it is best assessed whilst removing the transducer from the vagina at the conclusion of the scan, gently fanning side to side to assess for nodules. 1
tips and tricks to assessing for de
- if the ureters are dilated or extensive pelvic endometriosis is present, the scan should be extended to include a transabdominal assessment of the kidneys. 2
- when endometriosis is present, dynamic assessment and pressure in the posterior compartment can be painful, as such, a throughout explanation of the procedure and frequent checking on the patient’s comfort are a must. over the counter pain relief (such as ibuprofen) can be beneficial to some people post scan.
- mobility of the organs can be affected by the position of the ovaries, body habitus and pain tolerance; care should be taken when labelling an ovary immobile to insure this is pathological rather than technical
- adhesions within the pelvis can be due to prior (or current) pelvic infection, surgery or endometriosis. 1
- if using a three-dimensional mechanical transvaginal transducer, the steering or tilt function can be employed to assess places otherwise difficult to access comfortably (e.g. distal rectum)
- extensive deep endometriosis can cause significant distortion of the normal pelvic anatomy; if the exact location of a nodule cannot be definitively determined, describing as being located in the “anterior compartment” or the “posterior compartment” is most clinically helpful .1
- one-third of women with a previous caesarean section will have adhesions in the vu space1
- free fluid in the pod this can be used as an acoustic window to visualise small (even superficial) lesions within the posterior compartment
references
- s. guerriero, g. condous, t. van den bosch, l. valentin, f. p. g. leone, d. van schoubroeck, c. exacoustos, a. j. f. installé, w. p. martins, m. s. abrao, g. hudelist, m. bazot, j. l. alcazar, m. o. gonçalves, m. a. pascual, s. ajossa, l. savelli, r. dunham, s. reid, u. menakaya, t. bourne, s. ferrero, m. leon, t. bignardi, t. holland, d. jurkovic, b. benacerraf, y. osuga, e. somigliana, d. timmerman. systematic approach to sonographic evaluation of the pelvis in women with suspected endometriosis, including terms, definitions and measurements: a consensus opinion from the international deep endometriosis analysis (idea) group. (2016) ultrasound in obstetrics & gynecology. 48 (3): 318. doi:10.1002/uog.15955– pubmed
- mathew leonardi, george condous. how to perform an ultrasound to diagnose endometriosis. (2018) australasian journal of ultrasound in medicine. 21 (2): 61. doi:10.1002/ajum.12093
- mathew leonardi, george condous. a pictorial guide to the ultrasound identification and assessment of uterosacral ligaments in women with potential endometriosis. (2019) australasian journal of ultrasound in medicine. 22 (3): 157. doi:10.1002/ajum.12178
- jing fang, sofie piessens. a step‐by‐step guide to sonographic evaluation of deep infiltrating endometriosis. (2018) sonography. 5 (2): 67. doi:10.1002/sono.12149