normal laminar flow: in the peripheral arteries of the limbs, flow will be triphasic with a ‘clear spectral window’ consistant with no turbulence. the spectral window is the area under the trace.
stenotic arterial flow.
nb: if the stenosis is short, there can be a return to triphasic flow dependant on the ingoing flow and quality of the vessels. presence of triphasic flow does not exclude proximal stenosis in a symptomatic patient.
arterial occlusion schematic.
monophasic flow: will be present approach an occlusion (or near occlusion). the degree of loss of phasicity will be dependant on the quality of collateral circulation bridging the pathology.
distal post-stenoic normal laminar arterial flow
biphasic flow.
distal post-stenoic normal laminar arterial flow
diminished flow.
triphasic flow
triphasic flow: normal flow pattern in a vessel with minimal arteriosclerosis in the area being investigated. the phases are indicative of the elasticity of the vessel and the downstream resistance.
optimise your spectral (pulsed) doppler settings.
biphasic flow
as the name suggests, there are 2 phases/components to the spectral doppler trace.
the loss of the 3rd phase from the triphasic waveform indicates a degree of disease.
there are 2 presentations of biphasic flow, each indicating differnet pathologies.
biphasic flow 1: loss of the 3rd phase is generally an indication of the loss of elasticity of a vessel.
biphasic flow 2: the constant forward flow during diastole suggests a decrease in downstream resistance. this may be the result of a degree of vasodilation in response to compromised flow.
monophasic flow
as with biphasic, monophasic has 2 presentations, both indicating significant disease.
no diastoloc flow at all indicates an approaching (downstream) significant stenosis or occlusion.
almost vein-like flow throughout systole and diastole. this is downstream of an occlusion with flow reconstituted via a collateral network. if you see this flow but found no upstream pathology you should rescan the upstream system.
monophasic flow 1: approaching an occlusion (or an almost occluded segment).
monophasic flow 2: post severe stenotic disease or occlusion, with flow reconstituted via a collateral network. loss the cardiac induced phasicity induces the “venous-like” flow.
stenosis criterion
profile of a stenosis
the flow through most stenoses behaves like a flame on a candle with the hottest point (highest velocity) not at the wick(plaque) but at the tip of the flame. utilise the aliasing in colour doppler to identify the highest velocity.
in this diagram the velocity should be measured at point ‘b’ rather than point ‘a’. see the 2 example images opposite.
1st velocity image is at point ‘a’.
2nd velocity image is at point ‘b’.
the difference in velocity is evident. higher, immediately distal to the plaque.
occlusions
it is important to make note of:
the postion of the occlusion relative to landmarks (such as the groin or knee crease).
the length of the occlusion.
the presence of collateral vessels.
for example:
there is a 5cm occluded segment of the sfa 15cm below the groin crease, with large collaterals bridging the occlusion.
occluded distal sfa (green) with large collateral vessels arising and wrapping over the femoral vein.
aneurysms
a calcified fusiform aneurysm of the superficial femoral artery.
ultrasound image- pseudo-aneurysm: a post traumatic aneurysm of the common femoral artery. the most common cause is following cannulation if the artery, particularly angiography.
if a pseudo-aneurysm with a narrow neck, is discovered soon after its formation (eg post angiography), graded compression using ultrasound may be employed to seal the neck.
embolus
an embolus is a travelling thrombus.
they may occur spontaneously or post trauma/surgery.
sources
spontaneous – clot
cardiac – clot
post surgical – fat or clot
long bone fracture – fat embolus
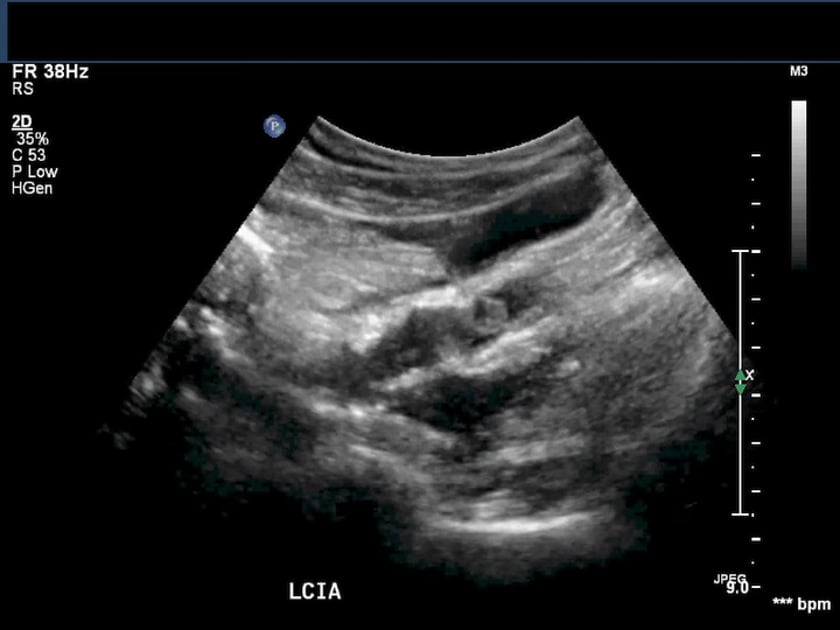
ultrasound of iliac artery mobile thrombus (embolus)
ultrasound of a large iliac mobile embolus in the external iliac artery in this atheromatous vasculopath patient. bacteraemic in icu.